This website is intended for healthcare professionals only.
Take a look at a selection of our recent media coverage:
4th March 2024
While a significant proportion of patients with myocardial infarction are prescribed clopidogrel, common genetic variants mean that some people – and more from certain ancestry groups – may not see its preventative benefit.
Here, Dr Emma Magavern, clinical research fellow for the Centre of Clinical Pharmacology and Precision Medicine at William Harvey Research Institute, Queen Mary University of London, UK, discusses her most recent findings and the value of clinicians adopting pre-emptive pharmacogenomic testing.
As clinicians, we know that there is inter-individual variability in medication response. Different people respond differently to the same medication; some take medication and do not experience the intended benefit, and some people unfortunately experience adverse drug reactions (ADRs). Some of this variability in response is due to genetics.
We already use other information known to impact on risk of ADRs from a medication in our clinical practice. Examples include checking liver and renal function before prescribing medicines.
By using information on very common genetic markers to inform prescribing, we can optimise the benefits of medications and minimise the risk of side effects. This area, known as pharmacogenomics, has however been slow to enter mainstream clinical practice.
The recently published PREPARE trial showed that a pre-emptive pharmacogenomic testing approach, where the genotype informs prescribing, can decrease ADRs by one-third in a multi-centre prospective clinical trial setting.1
ADRs pose significant problems for patients and take a large toll on healthcare systems. Studies estimate ADRs are responsible for 6.5% of hospital admissions in the UK and cost more than £2bn a year to the NHS.2,3 So there is clearly much room for improvement.
People from certain ancestry groups may have a higher risk of experiencing a side effect or not benefiting from medication due to common genetic variants. An example is illustrated by the use of clopidogrel after a myocardial infarction.
Clopidogrel is a commonly prescribed P2Y12 inhibitor used for secondary prevention after an initial ischaemic event.4 It is a prodrug and must therefore be activated in the body, via metabolism by cytochrome P450 2C19 (CYP2C19) in the liver, to achieve potency. Studies have shown that 60–70% of people who suffer from a myocardial infarction are prescribed clopidogrel.5
The CYP2C19 enzyme is encoded by the CYP2C19 gene, which is highly polymorphic.6 People with CYP2C19 loss of function (LOF) variants have higher on-treatment platelet reactivity with clopidogrel and are at a greater risk of secondary ischaemic events.7
LOF variants in CYP2C19 are common – present in approximately one in three people of European ancestry.7 Therefore, genetic variants resulting in individuals not being able to activate clopidogrel are common.
However, these variants are even more common in certain ancestral groups. Genetic changes that lead to poor activation of clopidogrel are most common in Asian and Oceanic ancestry groups.8
So, these ancestry patients have a higher risk of clopidogrel being ineffective than European ancestry participants, in whom antiplatelets were predominantly trialled, and therefore might benefit most from the use of genetics to help determine clopidogrel safety and efficacy (see Table 1 below).
Few studies have linked genetic data from under-represented populations with medication exposure and health outcome data. The only study with a substantial Asian population was focused on stroke rather than myocardial ischaemia and undertaken in east Asia.
Table 1. Studies supporting clopidogrel licensure as listed in the European Medicines Agency summary of product characteristics9–16

Table reproduced from Magavern E et al. JACC Adv 2023;2(7):100573. Copyright © 2023, The Authors. Open Access Article under the CC BY License.
The British-Bangladeshi and British-Pakistani populations in the UK are known to experience high rates of cardiovascular disease. The Genes & Health study recruited more than 50,000 people from this population and linked genotype data with national electronic health records data and primary care prescription records.17
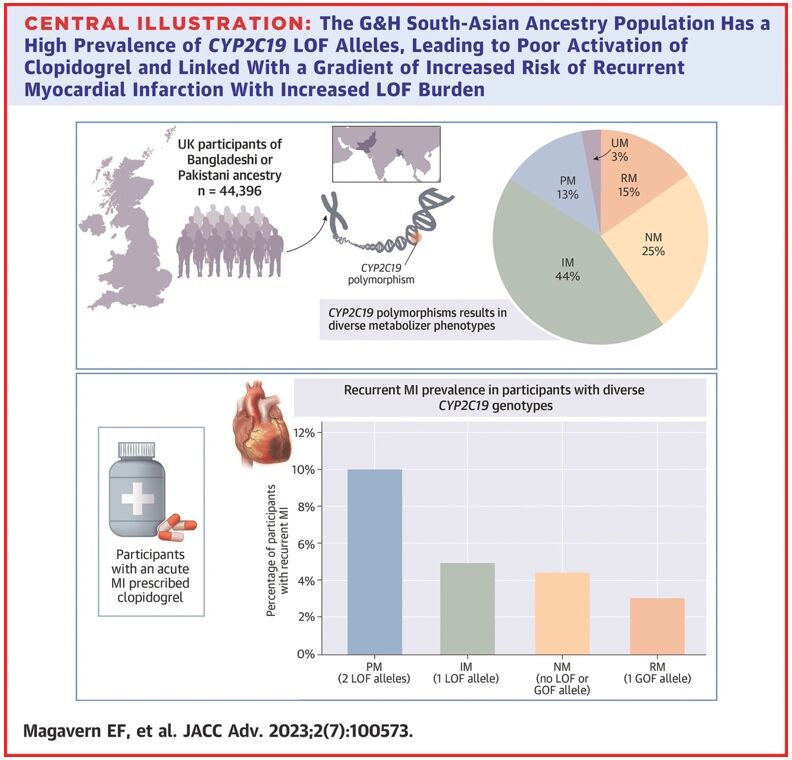
In an analysis of 44,396 participants, we found that 57% of people in this group had a CYP2C19 LOF variant.18 Of these, 13% had two copies of an LOF variant – one from each parent (Figure 1).
Figure 1. Prevalence of CYP2C19 LOF alleles in the Genes & Health study’s South-Asian ancestry population
Reproduced from Magavern E et al. JACC Adv 2023;2(7):100573. Copyright © 2023, The Authors. Open Access Article under the CC BY License.
We identified people in this group who had experienced a myocardial infarction and were prescribed clopidogrel by their GP (697 participants). Those with a recurrent myocardial infarction were almost four-times more likely to have two LOF CYP2C19 alleles as compared with none. A total of 69% of participants who had a myocardial infarction were prescribed clopidogrel.18
This study showed how common genetic resistance to clopidogrel is in this population. It also demonstrated the widespread use of clopidogrel and linked genetic resistance with a higher risk of recurrent myocardial infarction in this population for the first time, using real-world data.
While a precision prescribing approach using CYP2C19 testing would benefit patients from all ancestries, it would disproportionately benefit the South-Asian ancestry population due to the higher prevalence of both coronary artery disease and genetic resistance to clopidogrel in this population.
Genetic testing may soon be available within the NHS to determine if stroke patients would benefit from clopidogrel.19 This means that some patients might already know their CYP2C19 genotype when they present with a secondary ischaemic event.
This information could subsequently be used to administer the most effective medicine and reduce their risk of further ischaemic events.
For pharmacogenetic testing to benefit patients who have had a myocardial infarction, several things must occur:
There should also be discussion with the public around this use of genetic testing, to raise awareness and design clinical pathways fit for purpose. These dialogues must include historically under-represented ancestry groups and build trust.
The goal is to make genetic testing possible in routine clinical care to help optimise antiplatelet choice after an ischaemic event and to ensure better outcomes for all, with a particular focus on improving health equality for the British South-Asian ancestry population.
Emma Magavern MD MSc MRCP
Clinical Research Fellow, Centre of Clinical Pharmacology and Precision Medicine, William Harvey Research Institute, Queen Mary University of London, UK
30th August 2023
A genetic study has revealed how the use of clopidogrel in British patients of south Asian ancestry appears to be less effective at preventing recurrent myocardial infarction than in those of European descent.
The study, which was published in the journal JACC: Advances, sought to assess the prevalence of common CYP2C19 genotype polymorphisms in a British south Asian population and correlate these with recurrent myocardial infarction risk in participants prescribed clopidogrel.
Researchers used data from the East London Genes & Health (ELGH) database – a community-based, long-term study of health and disease in British Bangladeshi and British Pakistani people in east London. ELGH incorporates cutting-edge genomics with electronic health record data linkage and targeted recall-by-genotype studies.
Using data from 44,396 individuals, researchers found a high prevalence (57%) of intermediate or poor CYP2C19 metabolisers, with at least one loss-of-function CYP2C19 allele.
In addition, the prevalence of poor metabolisers, characterised by two CYP2C19 loss-of-function alleles was 13%, which was higher than that in previously studied European (2.4%) and central/south Asian populations (8.2%).
In the cohort, 69% were diagnosed with an acute myocardial infarction and prescribed clopidogrel. Poor metabolisers were found to be significantly more likely to have a recurrent myocardial infarction (Odds ratio, OR = 3.1, 95% CI 1.2 – 8.1, p = 0.019).
Dr Emma Magavern, lead author from Queen Mary University of London, said: ‘This study highlights the importance of using genetics to determine who can benefit from clopidogrel after a heart attack, and how not doing so is likely to disproportionately disadvantage specific groups, such as south Asians.
‘British peoples of south Asian ancestry suffer from high rates of cardiovascular disease and therefore have both a high risk of needing an anti-platelet medication and a high risk of treatment failure with clopidogrel.’
The P2Y12-inhibiting agent clopidogrel, which can be used post-myocardial infarction to reduce the risk of a second infarction, as well as to lower the risk of bleeding following a percutaneous coronary invention, is metabolised by the hepatic enzyme CYP2C19. This transformation converts the inactive pro-drug into an active metabolite.
26th January 2023
Chinese researchers from the University of Shanghai have reported that the combination of ticagrelor and aspirin reduced the incidence of ischaemic major adverse cardiac events (MACE) compared to clopidogrel and aspirin, following the implantation of emergency drug-eluting stents in patients with a ST-elevation myocardial infarction.
The use of dual anti-platelet therapy combining aspirin and a P2Y12 receptor inhibitor reduces recurrent MACE in patients undergoing a percutaneous coronary intervention (PCI) with drug-eluting stents. Despite the proven value of this combination treatment, it has become clear that continued high on-treatment platelet reactivity to adenosine diphosphate, is associated with adverse clinical events. In fact, there is evidence to suggest that between 4 and 30% of patients treated with clopidogrel fail to show an adequate platelet response. Moreover, use of ticagrelor has been shown to exhibit a lower level of high on-treatment platelet reaction in comparison to clopidogrel. Despite these findings, the reason for high on-treatment high residual platelet reactivity remain unclear but elevated levels of fibrinogen despite treatment with drugs such as clopidogrel have been found to be independently associated with the risk of ischaemic myocardial injury following elective PCI in patients treated with clopidogrel.
In the current study, the Chinese team examined the impact of fibrinogen on residual platelet reactivity after an emergency drug-eluting stent implantation in patients treated with either aspirin and clopidogrel, or aspirin and ticagrelor, over a 12-month period following their stent implant. The team used a prospective design and included patients undergoing PCI and who were prescribed aspirin 100 mg with clopidogrel 75 mg daily or aspirin and ticagrelor 90 mg twice daily for at least 12 months. The researchers measured both on-treatment platelet reactivity and the fibrinogen concentration and which was divided into quartiles. The endpoint of interest was ischaemic MACE, which was a composite of several adverse cardiovascular outcomes e.g., unplanned revascularisation, ischaemic stroke.
Ticagrelor and MACE
A total of 919 patients aged between 62.9 and 65 years and of whom, between 76.8 and 83.8% were male, were included in the final analysis, with 55.8% prescribed clopidogrel.
The rates of MACE were significantly elevated among patients prescribed clopidogrel compared to ticagrelor (HR = 1.72, 95% CI 1.21 – 2.43, p = 0.004).
Overall, MACE occurred in 14.3% of the entire cohort and the highest risk was found in patients with high residual platelet reactivity and those in the highest quartile of fibrinogen levels (HR = 10.02, 95% CI 4.67 – 21.46, p < 0.001).
The authors concluded that both a high fibrinogen level and high residual platelet reactivity could be used to identify patients at risk of an ischaemic event over a 12 month period and suggested that ticagrelor provided a better prognosis than clopidogrel.
Citation
Yao Y et al. The impact of high on-treatment platelet reactivity and fibrinogen levels on ischemic events in patients with ST elevation myocardial infarction: a prospective observational study. Int J Clin Pharm 2023
IMPORTANT LINKS
MORE FROM COGORA
© Cogora 2025
Cogora Limited. 1 Giltspur Street, London EC1A 9DD
Registered in the United Kingdom. Reg. No. 2147432




