Professors Carl Philpott and Claire Hopkins, joint leaders of the landmark MACRO programme – the most extensive clinical investigation into the management of chronic rhinosinusitis to date – discuss how the results challenge long-held assumptions about the roles of antibiotics and surgery and consider the implications for patients, clinicians and future care pathways.
Chronic rhinosinusitis is a common, chronic inflammatory condition that affects the paranasal sinuses and nasal passages. Symptoms include nasal discharge, nasal congestion, a decreased sense of smell and facial pressure or pain lasting for more than 12 weeks. It can significantly impact patients’ quality of life, ability to work, social interactions and daily activities.1,2
Chronic rhinosinusitis is phenotypically classified according to the presence or absence of nasal polyps. Both phenotypes exhibit considerable heterogeneity and are further subdivided into distinct endotypes based on histopathological and inflammatory features of the nasal mucosa.3
Historically, disease with polyps has been associated with a predominantly type 2 inflammatory response, characterised by elevated interleukin levels, immunoglobulin E levels above 100 IU/L and/or eosinophil counts exceeding 0.15 x109. Conversely, disease without polyps has been viewed as more typical of a type 1 inflammatory profile.3
Antibiotics vs surgery for chronic rhinosinusitis
Aside from the evidence supporting steroid nasal sprays and saline irrigations, there has been a lack of randomised controlled trial data on the use of antibiotics and sinus surgery. This has led to sinus surgery being regarded as a procedure of limited clinical effectiveness in chronic rhinosinusitis. Patients have also expressed frustration that surgery is only considered after medical therapies have been tried and may only provide a temporary solution.4
Discussion with GPs and ear, nose and throat (ENT) surgeons revealed major uncertainty about the role of longer courses of antibiotics and the use of oral steroids. Their views on the timing of surgery were that it remained unclear, and they felt that the uncertainty about the net long-term benefits of surgery made balancing benefits and risks more difficult.5
Our analysis of general practice data showed high rates of repeated antibiotic prescriptions among some patients with chronic rhinosinusitis in primary care, with nearly one in 10 receiving five or more chronic rhinosinusitis-related courses in a five-year period.6
Defining best management in chronic rhinosinusitis: the MACRO trial
The MACRO programme was established in 2016 when the UK National Institute of Health Research awarded £3.2m to define the best management of adults with CRS.
The programme comprised three workstreams:
- Workstream 1: health informatics, health economics and qualitative research
- Workstream 2: delivery of the MACRO trial
- Workstream 3: consensus-building and dissemination activities.
The MACRO trial commenced in late 2018 and aimed to compare the clinical effectiveness of endoscopic sinus surgery with a three-month course of intranasal clarithromycin, alongside standard intranasal medication, in adults with chronic rhinosinusitis with and without polyps.7
Conducted as a pragmatic, three-arm randomised, placebo-controlled phase 4 trial, the study recruited 514 adults with chronic rhinosinusitis from 20 secondary and tertiary care sites across the UK.
All participants were aged 18 or over and remained symptomatic despite appropriate medical therapy comprising intranasal corticosteroids, saline irrigation and a short course of antibiotics. Of those enrolled, 181 were female (35%) and 333 were male (65%); 410 had chronic rhinosinusitis with nasal polyps (80%) and 104 had it without nasal polyps (20%).
Included participants were randomly assigned (1:1:1) to one of three treatment arms:
- Arm 1: endoscopic sinus surgery within six weeks of randomisation (n=171)
- Arm 2: clarithromycin 250 mg twice a day for two weeks, then 250 mg once a day for 10 weeks with intranasal medication (n=172)
- Arm 3: placebo with intranasal medication (n=171).
Participants in all three groups continued to use intranasal medication during the study.
Outcome measures
The primary outcome of the trial was the 22-item Sino-Nasal Outcome Test (SNOT-22) quality-of-life questionnaire completed six months after randomisation. Lower scores indicated a better sinonasal-related quality of life.
Secondary outcome measures included the Lund-Kennedy endoscopic score, Lildholdt polyp score, peak nasal inspiratory flow rate (PNIF), peak expiratory flow rate (PEFR) and generic health-related quality of life scores (Short Form-12 and EuroQol 5-Dimension 5-Level visual analogue scale).
The Sniffin’ Sticks TDI smell test, which assesses olfactory function across subtests for olfactory threshold (T), odour discrimination (D) and odour identification (I), was also used.
What did the results show?
At six months from randomisation, SNOT-22 scores were significantly lower in the endoscopic sinus surgery group than the clarithromycin group (adjusted mean difference –18.13; 98·33% CI –24·26 to –11·99; p<0.0001) and the placebo group (–20.44; 98·33% CI –26.42 to –14.46; p<0.0001).
SNOT-22 scores did not significantly differ between participants assigned to clarithromycin versus placebo (–3.11; CI –8.56 to 2.33; p=0.17).
The secondary outcomes also showed significant differences in favour of endoscopic sinus surgery at six months, except for PEFR and PNIF, which did not provide evidence of differences between the groups.
Regarding improvements in participants’ sense of smell, the trial showed a significantly greater increase in TDI scores six months after randomisation in the surgical group compared to the placebo. However, only 40% of those in the surgical arm achieved the minimum clinically important difference of 5.5 points on the TDI score.
Regarding further treatment, no significant differences were observed between the groups, and Asthma Control Test scores remained similar throughout follow-up.
Adverse events were rare across all groups, with 10 serious adverse events in nine participants: two events in two participants (1%) in the clarithromycin group, three events in three participants (2%) in the placebo group, and five events in four participants (2%) in the surgery group. None of these events were fatal, and all resulted in discharge without any lasting sequelae.
Endoscopic surgery enhanced quality of life in patients with and without nasal polyps compared to clarithromycin and placebo. Additionally, when comparing disease endotypes, surgery proved effective in both main endotypes, with a stronger effect observed in type 2 inflammatory disease.
Clarithromycin did not show a significant effect on SNOT-22 in either subgroup, but there was a trend toward significance in non-type 2 chronic rhinosinusitis participants.
Guiding the future management of chronic rhinosinusitis
The MACRO trial findings indicate that long-term macrolides such as clarithromycin should not be used routinely in patients in primary care or secondary care, especially when the endotype is not determined.
Although the subgroup was underpowered, clinicians can consider clarithromycin treatment for patients with non-type 2 chronic rhinosinusitis. However, we plan to gather more evidence regarding its effectiveness in this subgroup.
The results of the trial should provide clinicians and commissioners with confidence in offering surgery as a treatment option to adults with chronic rhinosinusitis without adequate response to intranasal treatments. Furthermore, many trial participants are remotely monitored each year for five years, and we plan to publish these long-term results in 2029 when data collection ends.
We now propose a new pathway for chronic rhinosinusitis patients from primary to tertiary care, as shown in Table 1 below. The pathway highlights the key messages above, particularly to ensure that patients are offered sinus surgery without delay if their symptoms do not respond to intranasal medication.
Table 1. Proposed chronic rhinosinusitis care pathway from primary to tertiary care
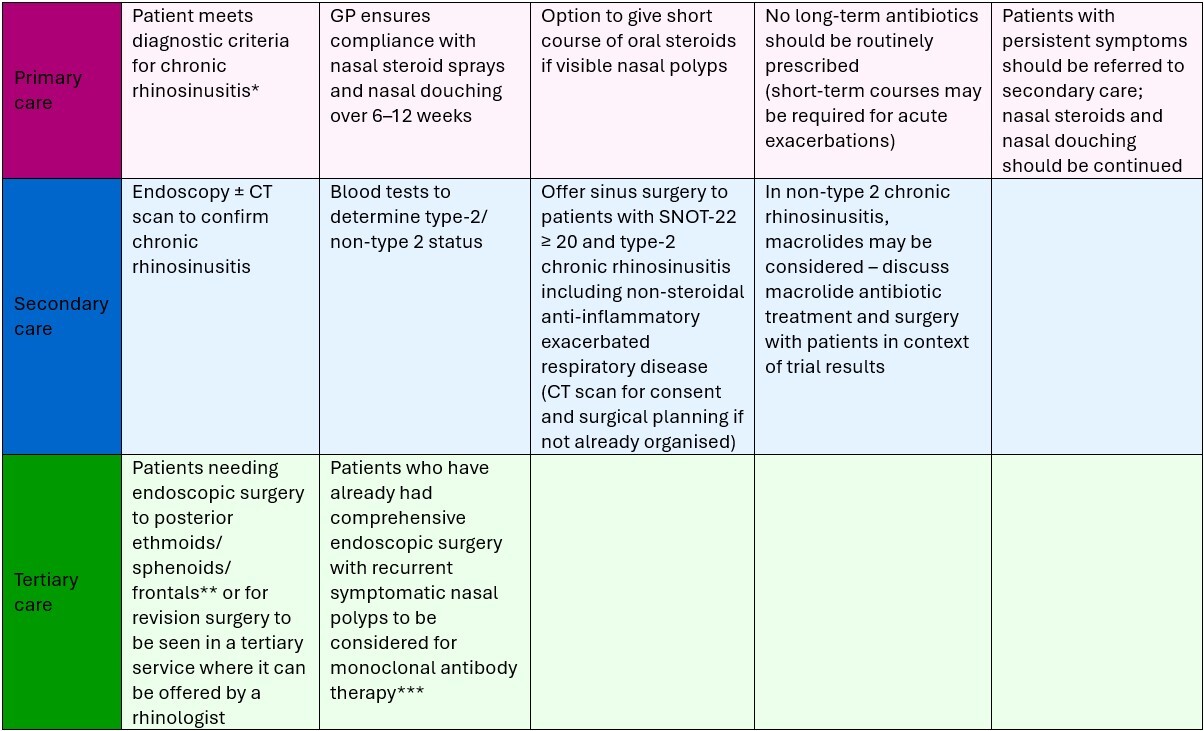
* According to reference 2; ** According to the Getting it Right First Time endoscopic sinus surgery pathway; *** Subject to National Institute for Health and Care Excellence pending approval.
Implementing the MACRO trial findings in clinical practice could help to reduce the current number of unnecessary antibiotic prescriptions in chronic rhinosinusitis. Considering the significance of antibiotic resistance, this approach might also lower costs related to prescriptions and appointments by enabling patients to access endoscopic sinus surgery earlier in their treatment pathway.
Authors
Professor Carl Philpott MB ChB DLO FRCS(ORL-HNS) MD PGCME
Professor of rhinology and olfactology, Norwich Medical School, University of East Anglia, and honorary consultant rhinologist and ENT surgeon, James Paget University Hospitals NHS Foundation Trust, UK
Professor Claire Hopkins BM BCh DM (Oxon) FRCS(ORL-HNS)
Consultant ENT surgeon, Guy’s and St Thomas’ NHS Foundation Trust, and professor of rhinology, King’s College London, UK
References
- Erskine SE et al. Chronic rhinosinusitis: patient experiences of primary and secondary care - a qualitative study. Clin Otolaryngol 2016;41(1):8–14.
- Fokkens WJ et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020;58(Suppl S29):1–464.
- Wang M et al. New insights into the endotypes of chronic rhinosinusitis in the biologic era. J Allergy Clin Immunol 2025;156(1):51–60.
- Vennik J et al. Chronic rhinosinusitis: a qualitative study of patient views and experiences of current management in primary and secondary care. BMJ Open 2019;9(4):e022644.
- Vennik J et al. Management strategies for chronic rhinosinusitis: a qualitative study of GP and ENT specialist views of current practice in the UK. BMJ Open 2018;8(12):e022643.
- Hopkins C et al. Antibiotic usage in chronic rhinosinusitis: analysis of national primary care electronic health records. Rhinology 2019;57(6):420–9.
- Philpott C et al. The clinical effectiveness of clarithromycin versus endoscopic sinus surgery for adults with chronic rhinosinusitis with and without nasal polyps (MACRO): a pragmatic, multicentre, three-arm, randomised, placebo-controlled phase 4 trial. Lancet 2025;406(10506):926–39.