





Chronic obstructive pulmonary disease (COPD) is a chronic disease that affects different systems of the body. Heart failure and morbidity is strongly associated with this disease.1 COPD is closely monitored by pulmonary function tests and imaging techniques, such as CT of the thorax. One of the main concerns is whether a patient will develop respiratory deficiency and will require life-long oxygen supplement on a 24-hour basis. Moreover, these patients tend to develop different patterns within the lung parenchyma such as emphysema or bronchiectasis, or both. The damage that develops (phenotype) depends on the patient’s genotype. Lack of α1-antitrypsin if any also plays a role in the development of emphysema or bronchiectasis.
Emphysema is differentiated as homogenous or heterogenous; however, one of the main issues is the lack of definition for each diagnosis. Lung volume reduction surgery (LVRS) is known to be an invasive therapeutic option for some patients, for others currently we have different minimal invasive techniques.2 Based on randomised controlled trials of medical management compared with LVRS (National Emphysema Treatment Trial (NETT)), LVRS-treated patients obtained improvements in lung function, symptoms, exercise tolerance and quality of life relative to the medically treated group.3 While long-term survival was improved, there was significant morbidity and mortality associated with surgery.3 The NETT study is considered as substantial evidence that benefits can be achieved with lung volume reduction (LVR) particularly those with heterogeneous emphysema and upper lobe predominance.3,4 Currently we can use different types of valves, coils, glue and thermal vapour ablation. Careful selection of a specific method is necessary before the application for each patient. The six minute walking test (6MWD), pulmonary function tests, nutrition, and special imaging techniques are used to assess each patient.
One of the most important issues is to present to the patient what to expect after each procedure; and that the main goal is improved quality of life. Moreover, that after every procedure constant monitoring and further non-medical rehabilitation with respiratory exercise and special nutrition is required. This article focuses on bronchoscopic thermal vapour ablation (BTVA), which uses heated water vapour to produce a thermal reaction that leads to an initial localised inflammatory response followed by permanent fibrosis and atelectasis. The remodelling results in reductions in tissue and air volume of the targeted regions of the hyperinflated lung.5 In an early preclinical animal study, higher doses were used than in humans and a dose-dependent volume reduction was observed. Slightly moderate evidence of serious risk was observed. Nineteen out of twenty animals studied survived the procedure; the one death was due to severe pneumothorax.6
Eleven patients underwent the current protocol confirmed using a lower dose of unilateral BTVA with an acceptable safety profile. The efficacy observed was modest and therefore a higher dose would be possible.7 Some words regarding the system. The system comprises a vapour generator and a vapour catheter (Figures 1 and 2). The vapour generator is an electronically controlled pressure vessel that generates and delivers precise amounts of energy as a heated vapour through the vapour (balloon) catheter and into a targeted lung segment (Figure 2). The BTVA procedure is performed in an operating room or advanced bronchoscopic suite suite under general anaesthesia with jet-ventilation respiratory model. However; the respiratory model can change from one patient to another. The vapour catheter is introduced through the bronchoscope into the targeted lung segment selected for treatment, where an occlusion balloon is then inflated and the pre-determined vapour dose (10 cal/g-1 tissue) is delivered. A high resolution CAT scan is performed at full inspiration and scans are obtained at pre-treatment, and at three and six months post-treatment. The total air volume of the target lobe is calculated at each time-point, and the change in air volume is related to pre-treatment (lobar volume reduction (LoVR)) and expressed as a percentage of pre-treatment volume.

Figure 1 The vapour ablation system
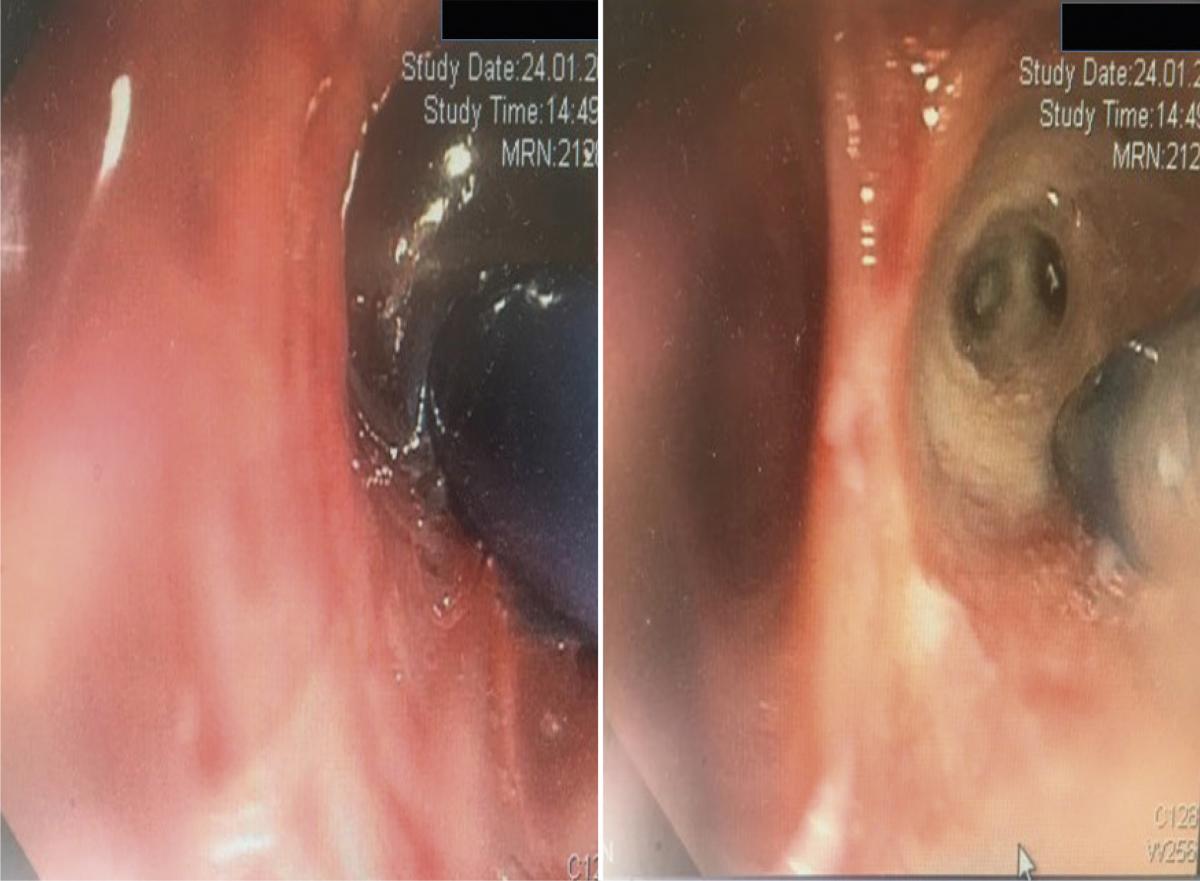
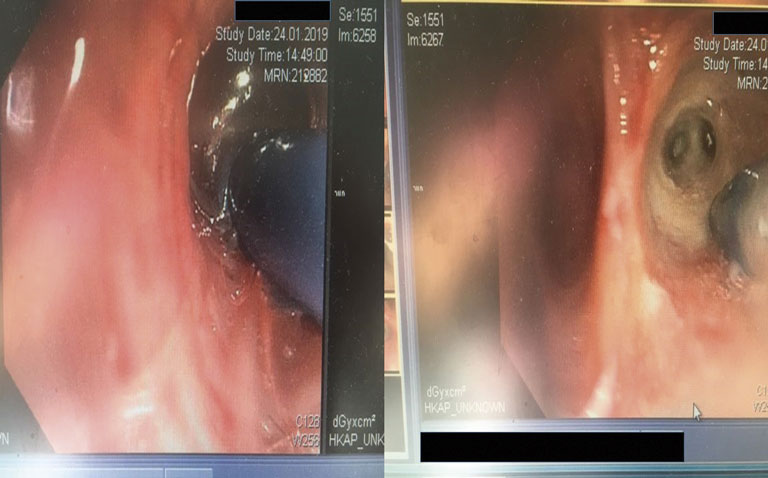
Figure 2 Left panel: The catheter inside the target lobe with the balloon dilated during the procedure. Right panel: The vapour catheter distally from the target lobe, and the ablated area
In addition to the imaging efficacy end-points, the BODE (body mass index, airflow obstruction, dyspnoea and exercise capacity) index are calculated for each patient.8 All patients are monitored in the hospital for a minimum of 24 h following BTVA. After discharge, patients return to their home and have a close follow-up visits at one, two and four weeks, and then at three and six months. Serious adverse events are defined as those that are either fatal, life-threatening, requiring or prolonging hospitalisation, or resulting in persistent or significant disability or incapacity. Upon follow-up, a number of tests are performed including: laboratory tests that include complete blood count, biochemistry and non-specific inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein (C-RP). Vital signs are also recorded during every visit. The mean procedure time is usually 29 min (range 12–58 min). Procedures are usually well-tolerated with most of the patients being discharged from the hospital within 24 hours. Until now there are no data for patients that required mechanical ventilation beyond the procedure time.
The average lobe volume loss from baseline in the treated lobes was 717.6 ± 78.8ml at three months and 715.5 ± 99.4ml at six months (p=0.001). This volume represents a 48% reduction in lobar volume in a recent reported study. It has been observed that the volume differences at six months are similar to those observed at three months. Compensatory hyperinflation of the contralateral lung has not been observed mainly due to the slow process of remodelling. Current data indicate that mean ± SE improvement in FEV1 has been observed at 139.1 ± 27.2ml (17%) at three months and 140.8 ± 26.3ml (17%) at six months (p=0.001). The mean ± SE improvement in SGRQ total score was 11.0 ± 2.3 and 14.0 ± 2.4 points at three and six months, showing no difference after three months’ observation. Today the largest difference has been observed in the activity domain (14.7 ± 2.8 points).
Dyspnoea (according to the mMRC index) improved by a mean of 0.9 ± 0.2 points at six months (p=0.001) and by at least one point in 63% of subjects. The average change in 6MWD has been observed between 23.5 ± 10.4m (p=0.029) and 46.5 ± 15.0m (p=0.001) at three and six months, respectively. The BODE score has been declined by 1.36 ± 0.27 and 1.4 ± 0.27 points at three and six months, respectively. Chronic obstructive pulmonary disease stage is improving with FEV1 by 120.4 ± 30.7ml in GOLD stage III (p=0.001) and 171.3 ± 47.1ml in GOLD stage IV profile(p=0.002) patients. Corresponding improvements in the SGRQ total score have been observed between 12.4 ± 2.7 points (p=0.001) and 16.3 ± 4.5 (p=0.002) points at three and six months, respectively. Until now, the adverse respiratory effects that have been observed are of respiratory origin, such as: exacerbation, pneumonia, lower respiratory tract infection, haemoptysis, and inflammatory reactions. The adverse effects can occur at different times after the procedure from day 1 to past day 90. There is also a report of patient death 67 days after the procedure due to end-stage COPD. This patient was re-admitted for an exacerbation of COPD. Usually all patients had their adverse effects resolved with standard medical management. Changes in the HRCT of all the patients were observed.
The inflammatory response in the targeted area was associated with different clinical symptoms including fatigue, cough, fever, dyspnoea, sputum, and haemoptysis. A localised inflammatory reaction (LIR) within the treated lobe is expected following BTVA, because this is the process that results in the atelectasis of a lobe and treatment of the patient. Unfortunately, the treated area will typically show infiltrates radiographically, that could be indistinguishable from pneumonia. Other symptoms or no syptoms might present at the same time, such as; fatigue, sputum, dyspnoea, fever, cough and haemoptysis. This inflammatory reactions appears to peak within the first 2–4 weeks and gradually resolves within 8–12 weeks of BTVA. (Figures 3 and 4) The patient need to be treated (that is, antibiotics and/or steroids) based on individual investigator clinical decisions. The LIR appears to be responsible for exacerbations and ‘pneumonia’, given the similarity or symptoms and radiographic findings. In the treated area a healing and repair process is characterised by fibrosis of the airways and parenchyma (that is, remodelling of the architecture of the lung). The atelectasis occurs distally from the treated region. The LVR is expected to increase elastic recoil by reducing the most compliant areas of the lung. Decompressing areas of healthy lung allows alveolar recruitment and improves the mechanical positioning of the respiratory muscles.
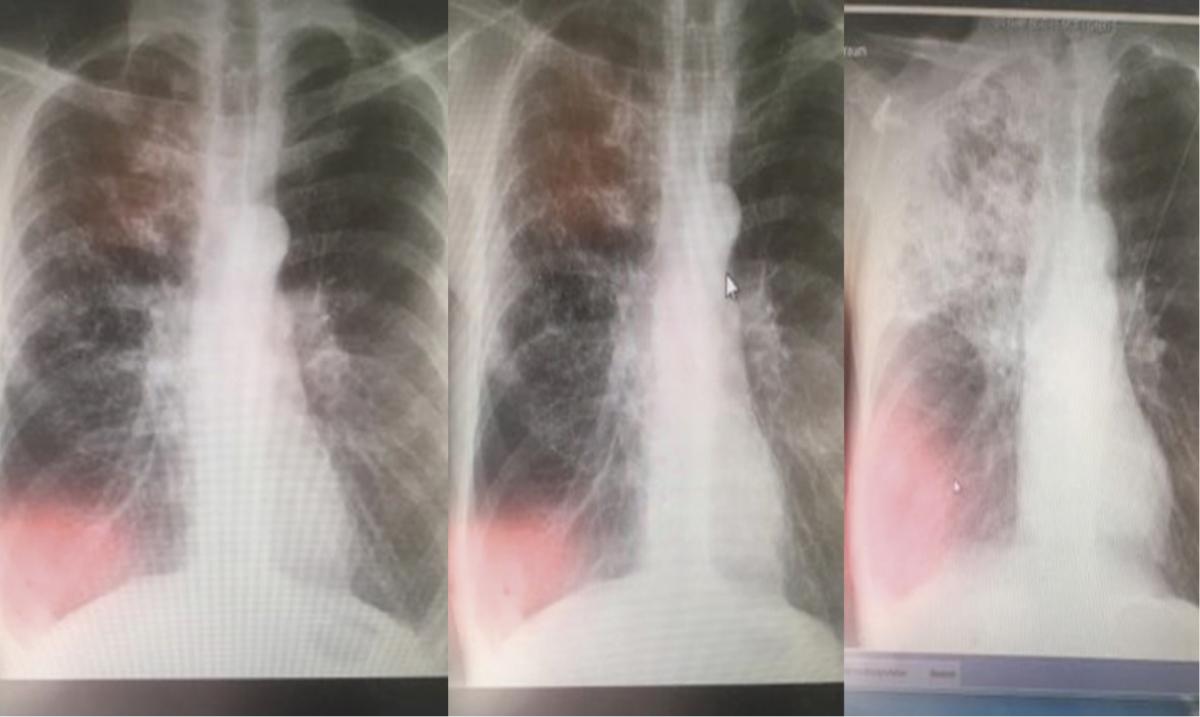
Figure 3 Radiographical findings on days 1, 3 and 30
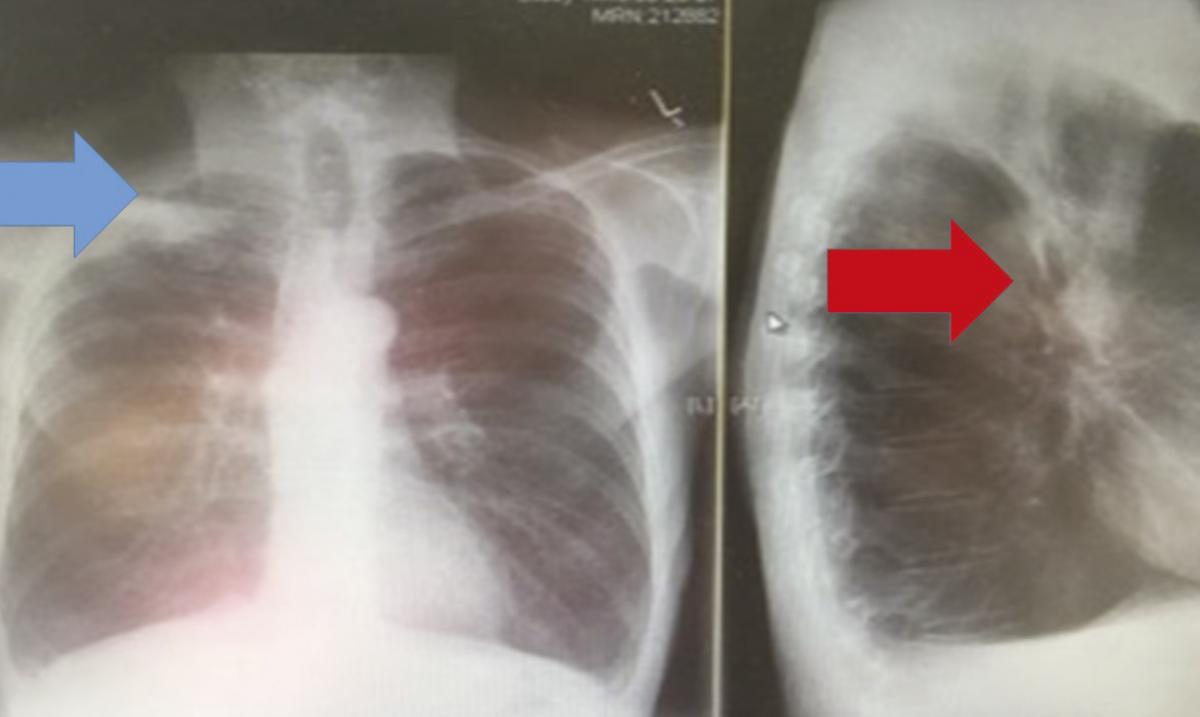
Figure 4 Radiographical findings on day 95 with target lobe (right upper lobe) atelectasis
Conclusions
In summary, BTVA treatment can be used successfully in patients with heterogeneous emphysema with upper lobe predominance. These patients may achieve clinically important improvements in physiology, quality of life and exercise tolerance following only a single session of unilateral BTVA. The procedure has been reported to be well tolerated, with all patients being discharged from hospital. Most of the inflammatory responses can be managed with standard care with the reasonable expectation of resolution over a few weeks. All treated patients have to go under careful selection with all the previously reported methods. In any case, the clinical condition of the patient plays a crucial role on the day of the admission and the patient must not have signs of exacerbation. Based on current data, BTVA has a favourable benefit–risk profile in COPD patients with heterogeneous emphysema.
References
1 van der Molen T, Kirenga BJ. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract 2015;69:513–4.
2 Berger RL et al. Lung volume reduction therapies for advanced emphysema: an update. Chest 2010;138:407–17.
3 Weinmann GG, Chiang YP, Sheingold S. The National Emphysema Treatment Trial (NETT): a study in agency collaboration. Proc Am Thoracic Soc 2008;5:381-4.
4 Lee SM et al; National Emphysema Treatment Trial Research Group. Methodologic issues in terminating enrollment of a subgroup of patients in a multicenter randomized trial. Clin Trials 2004;1:326–38.
5 Snell G et al. Bronchoscopic thermal vapour ablation therapy in the management of heterogeneous emphysema. Eur Resp J 2012;39:1326–33.
6 Emery MJ et al. Lung volume reduction by bronchoscopic administration of steam. Am J Respir Crit Care Med 2010;182:1282–91.
7 Snell GI et al. A feasibility and safety study of bronchoscopic thermal vapor ablation: a novel emphysema therapy. Ann Thoracic Surg 2009;88: 1993–8.
8 Celli BR et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med 2004;350:1005-12.
